
Treating Chronic Vestibular & Hearing Loss with Cutting Edge Implanted Devices
by James Phillips, PhD
Director of the Dizziness & Balance Center at University of Washington Medical Center
(Presented to Seattle Dizzy Group on 11/10/18)
This presentation gives an overview of vestibular and auditory prostheses including how the University of Washington Medical Center is currently evaluating these cutting edge implanted devices which will hopefully help to improve the quality of life for many with chronic vestibular and hearing loss.
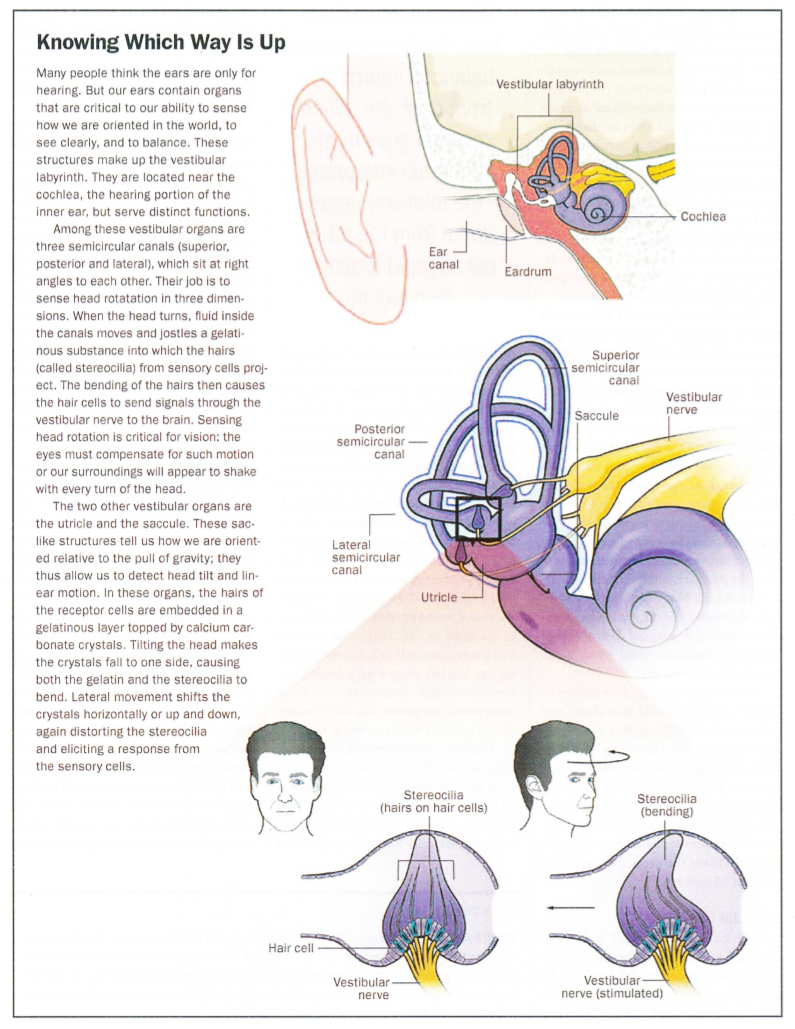
What is the Vestibular System?
- The vestibular system includes the structures in the inner ear that contribute to balance and orientation.
- It includes the nerves that relay balance and orientation information from the inner ear to the brain.
- It includes the neurons in the brain that make sense of that information, by combining information from a variety of sources:
- different parts of each inner ear
- from both ears
- from the visual system
- from the muscles and joints

What Parts of the Inner Ear are Parts of the Vestibular System?
- Semicircular canals
- Posterior canal
- Lateral canal
- Anterior canal
- Detect turning
- Otolith organs
- Utricle
- Saccule
- Detect front-back, right-left, up-down
- Detect tilt
- Vestibular Ganglia

What are the Semicircular Canals?
- 3 canals (posterior, lateral, anterior)
- Orthogonal
- Fluid filled
- Ampula
- Location of hair cells. (Our sense of balance starts with hair cells!).
- Like the hair cells in the cochlea for hearing
- Neural transduction
- Convert movement into neural signals
- Location of hair cells. (Our sense of balance starts with hair cells!).
How Do the Semicircular Canals Work?
- When you turn your head fluid moves in the semicircular canals.
- Each ampula contains a cupula, which billows when the fluid moves, which in turn bends the hairs of the hair cells.
- Gelatinous tongue
- Embedded hair cells
- Sense rotational acceleration
How Do the Otolith Organs Work?
- The otolith organs contain a gelatinous cap (otolithic membrane) and otoliths (otoconia, calcium carbonate crystals). They also contain hair cells.
- When we slide or tilt, the gelatinous cap deforms, and the hairs of the hair cells bend.
- Shear
- Sense of tilt and linear acceleration
What Happens When the Inner Ear Vestibular System Fails Bilaterally?
Both ears fail to work:
- No whirling vertigo
- Significant Disorientation
- Swimmy headed feeling
- Nausea and fatigue
- Conflicting sensory input
- Anxiety
- Cognitive Impairment
- Oscillopsia
- Failure to stabilize your eyes when you turn your head
- The visual world moves when you move
- Reduces your vision
- Postural and Gait Instability
Is There Compensation for Inner Ear Vestibular Loss?
- YES
- Over time we can compensate well for vestibular loss
- Especially true of children
- Our brains are designed to adjust for loss of input
- Compensation is dependent on learning:
- not to misinterpret sensory cues from a non-working vestibular system
- to use contextually appropriate cues
- to develop a general strategy that is adaptive over a range of situations
- to substitute useful information from other sensory systems:
- Somatosensory System
- Visual System
- Compensation requires sensory stability
- Defeated by change of fluctuation
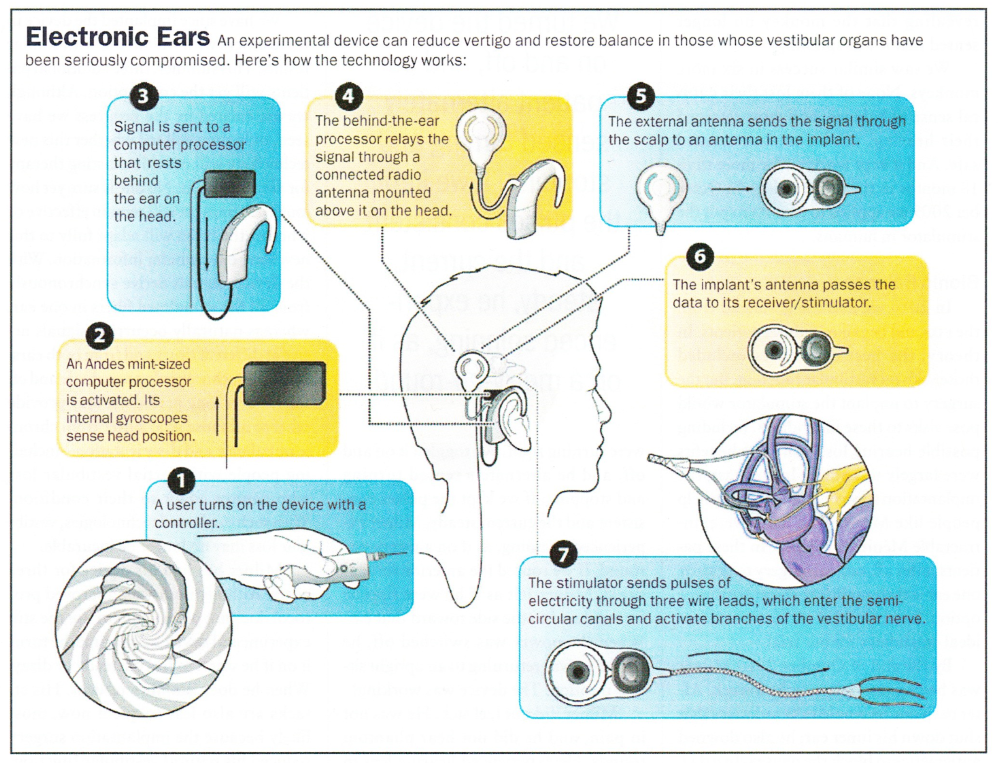
Can We Replace the Inner Ear Vestibular System?
Yes, with a vestibular prosthesis!
Who Could Be Treated with a Vestibular Prosthesis?
- Not patients with a single acute transient loss of function.
- Patients with bilateral loss of balance function.
- Often iatrogenic
- Exposure to ototoxic drugs
- Often iatrogenic
- Patients with uncompensated unilateral loss of balance function.
- Large numbers of patients do not adapt to a loss from one ear
- Patients with fluctuating balance function.
- Meniere’s Disease
- Extreme intermittent vertigo
- Destructive therapy
- Injected ototoxin, surgical ablation, nerve section
- These devices would take the place of a labyrinthectomy
- Destructive therapy
- Extreme intermittent vertigo
- Meniere’s Disease
- Usher Syndrome patients:
- Bilateral loss of balance dysfunction
- Combined with hearing loss
- Usher Syndrome patients may already have inner ear implants (cochlear implants for hearing loss).
- To effectively treat Usher Syndrome vestibular loss requires a combined vestibular and auditory implant.
UWMC Road to Human Trials
- Design a device to stimulate vestibular afferent fibers.
- Leverage a highly developed existing technology
- Cochlear implant
- Modify the software and hardware
- Create a minimally invasive electrode technology
- Create appropriate stimulation strategies
- FM not AM
- Partner with an existing Cochlear Implant manufacturer
- Leverage a highly developed existing technology
- Develop a simple surgical approach with the right target.
- Three semicircular canals
- Coherent rotational information
- Three semicircular canals
- Construct prototype devices.
- Identical to the final production device
UWMC Road to Clinical Trials
- Evaluate the device in animal model.
- Implanted devices in 14 rhesus monkeys
- Similar inner ear anatomy to humans
- Test in intact and lesioned animals
- Ideal model for unilateral and bilateral loss
- Evaluate risk
- Longitudinally evaluate inner ear function
- Using identical clinical tests to those that are used diagnostically in humans
- Longitudinally evaluate inner ear function
- Evaluate efficacy
- Longitudinally evaluate prosthetically elicited function
- Using clinically relevant behavioral and physiological measures
- Longitudinally evaluate prosthetically elicited function
- Implanted devices in 14 rhesus monkeys
- Test the device in human patients with vestibular loss.
- In 4 Meniere’s Disease patients
- Can the device restore vestibular function lost from the destructive treatment?
- In 4 Meniere’s Disease patients
- Modify our devices to create a combined cochlear and vestibular prosthesis.
- Test the new device in rhesus monkeys.
- Modify our existing FDA IDE to test patients with hearing and vestibular loss with the new combined implant.
- Test the new device in human patients with combined hearing and vestibular loss (2 additional patients, 6 total).
Turning the Implanted Device On
- Electrical stimulation with biphasic pulse trains
- Produces:
- Eye movements – eVOR (Vestibulo-Ocular Reflex)
- Body sway
- Sensation of motion
- Effective vestibular stimulation does not produce:
- Nausea
- Pain
- Sound sensation
- Facial nerve activation
UWMC Research Team Conclusions
- We know that a vestibular implant works!
- We have tested such a device in animals and humans.
- We have an existing approval to test these devices in patients.
- We have built a combined vestibular and cochlear implant.
- We are currently testing it in monkeys.
- We are working with the FDA to modify our existing human trial to test this new device.
- We are not the only ones doing this! (John Hopkins is researching similar implanted devices).
*This material regarding vestibular and auditory prosthetic technology is the intellectual property of the members of the device research team, the University of Washington, and Cochlear Ltd.*
More Information:
Conquering Vertigo article by James Phillips, PhD

James Phillips, PhD
Director of the Dizziness & Balance Center
University of Washington Medical Center
James Phillips, PhD, joined the faculty at the University of Washington in 1998 and is currently a research associate professor in the Department of Otolaryngology-Head and Neck Surgery. He is also the director of the Dizziness and Balance Center at the UW Medical Center, the Vestibular Diagnostic Laboratory at UWMC, and the Roger Johnson Clinical Oculomotor Laboratory in the Division of Ophthalmology at Seattle Children’s Hospital. Prior to joining UW, he earned a PhD in psychology and in physiology from the University of Washington. Dr. Phillips teaches in the Departments of Otolaryngology-HNS, Ophthalmology, and Speech and Hearing Sciences. He is a faculty research affiliate of the National Primate Research Center, the Virginia Merrill Bloedel Hearing Research Center, the Center on Human Development and Disability, and the Autism Center at the University of Washington. He is also a faculty affiliate of the Center for Navigation and Communication Sciences at the University of Rochester and the Center for Integrative Brain Research at Seattle Children’s Research Institute. He is on the Medical and Scientific Advisory Board of the Vestibular Disorders Association.
More information:
www.otolaryngology.uw.edu/faculty/james-o-phillips
*******
Presentation information is not meant to be taken as medical advice.
Presentations posted online may include discussion notes, links, images, and other information added by Seattle Dizzy Group.
*******
© Copyright 2018, Seattle Dizzy Group. All rights reserved.







[…] In 2018, we had guest speakers on the topics of “Mind Over What Matters” and “Postural Control & Balance” as well as “Gentle Yoga” and also “Vestibular & Auditory Prostheses.” […]
By: Together We Can Do So Much In 2019 | Seattle Dizzy Group on January 31, 2019
at 10:44 pm