
Persistent Postural-Perceptual Dizziness (PPPD)
by Morgan Kriz, DPT
Vestibular Physical Therapist
(Presented to Seattle Dizzy Group on 11/16/19)
This presentation gives an overview of Persistent Postural-Perceptual Dizziness (PPPD) which is a newly defined diagnostic syndrome described as a common chronic dysfunction of the vestibular system and brain that produces persistent dizziness, non-spinning vertigo and/or unsteadiness.
Visual distracting environments (such as supermarkets, large crowds, or watching TV) can be overwhelming and cause significant distress for people with a Vestibular Disorder. Once recognized, PPPD can be managed.
3PD
Persistent: symptoms present > 50% of the time for more than 3 months; but wax and wane. Can get better with distractions, progress later in the day.
Postural: exacerbated with upright posture (standing/walking); sudden movements
Perceptual: active (self generated movement) or passive movement (elevator, car) with exposure to moving (traffic) or complex visual stimuli (wallpaper, phone)
Dizziness: false or distorted sensations of swaying, rocking, bobbing, or bouncing of oneself (internal non‐spinning vertigo) or the surroundings (external non‐spinning vertigo)

RD-D2 & C3PO
Not a “New” Diagnosis
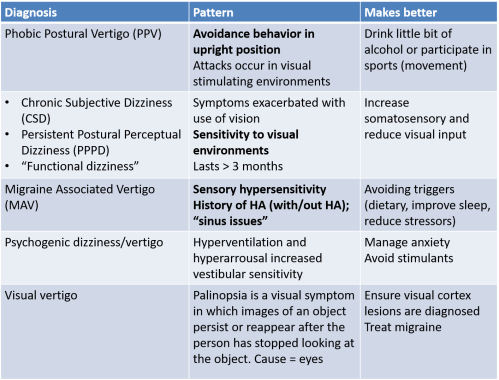
- Persistent Postural Perceptual Dizziness (PPPD, 3PD) – Dietrich and Staab 2014
- Chronic Subjective Dizziness (CSD) – Staab and Ruckenstein2004
- Visual Vertigo/Visual dependence/Space Motion discomfort (SMD) – Staab 2003
- Phobic Postural Vertigo (PPV) – Brandt and Dieterich 1986
- Mimic Post-Traumatic Stress Disorder (PTSD)
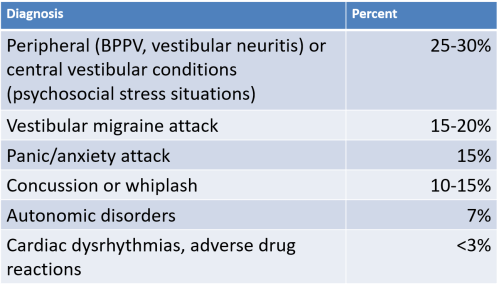
Prevalence of PPPD
- About 5% of the population develops “vestibular” dizziness per year (Hain):
- 0.05% = Mal Debarquement (0.5/1000 persons)
- 50% = land sickness “LDS”
- 1% = Vestibular Migraine
- 0.2% = Meniere’s Disease
- 10% = PPPD
How It Starts
Frequently at the beginning, there is an organic vestibular illness:
Medical Examination
- Normal eye exam
- Visual strain may contribute
- MRI/imaging = negative
- NO ABNORMAL INNER EAR
- * May start with an initial insult of inner ear years prior
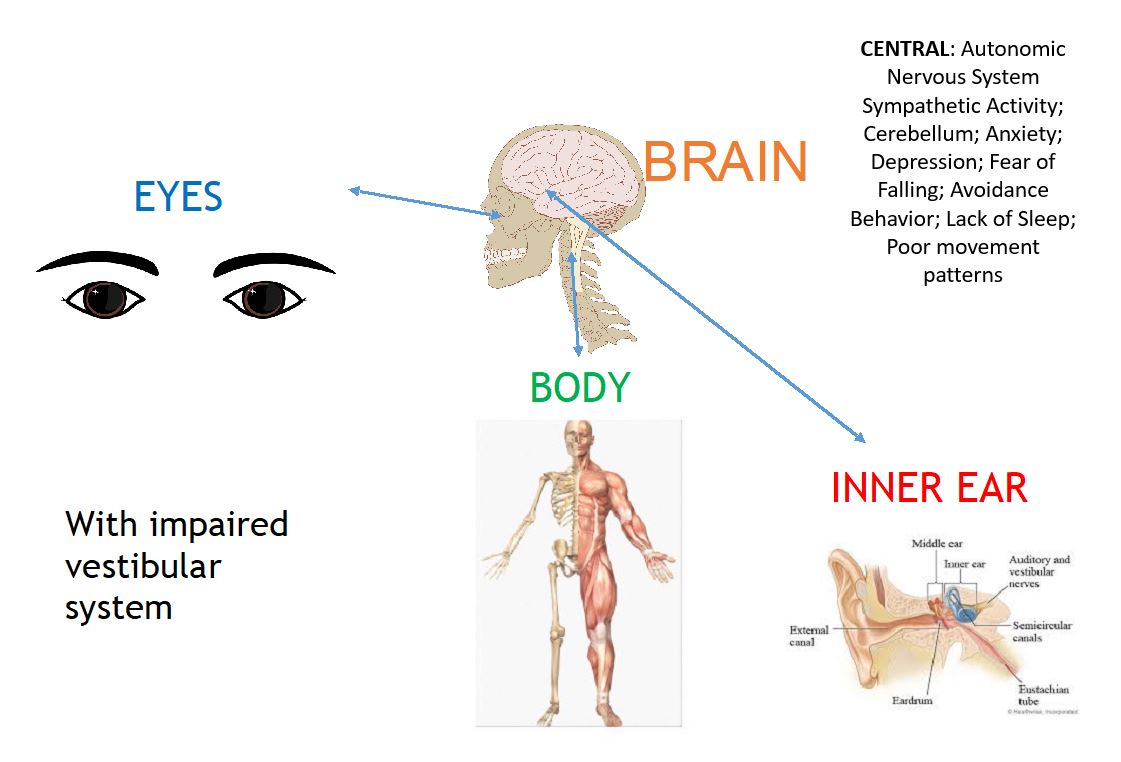
“Normal” Vestibular System

Impaired Vestibular System
Poor Recovery from Vestibular Illness

Misunderstanding
- PPPD is in fact a series of normal misunderstandings between the ears, spinal chord, eyes and brain. The signals have been mislead and misfired.
- It is all reversible!
Research Shows
- Emerging research suggests that it may arise from functional changes in postural control mechanisms, multi-sensory information processing, or cortical integration of spatial orientation and assessment
- Thus, PPPD is classified as a chronic functional vestibular disorder
- It is not a structural or psychiatric condition
Fight or Flight Initiated
- For this condition there is a strong link with anxiety and a subconscious underlying fear of the dizziness itself
- The body sensations are perceived with a ‘fright’
Fight or Flight Video
Anxiety and Fear
- THIS IS A NORMAL REACTION!
- It is not a psychiatric condition
- Neuro-otologic (vestibular-brain connection) condition with behavioral elements = not moving pattern
- Co-morbidities would make a person more “aware” of symptoms
- If the pattern continues = problem
PPPD
- If left unmanaged, emotions can delay the natural recovery process as chronic anxiety inhibits neuroplasticity
- Over time this can lead to increased anxiety and avoidance behaviors that perpetuate the PPPD condition
- Not using body or inner ear, and instead only visual = PPPD
Treatment Options
- Vestibular Physical Therapy Protocol
- Education on condition -> improve control -> reduce anxiety
- Evaluate for non-compensated vestibular hypofunction
- TRIGGERS (start journal)
- Reduce stress/GET SLEEP!
- Cervical spine contributions
- VOR adaptation
- Reduce visual dominance
- Cognitive and Behavioral Therapies
- Serotonergic Medications (serotonin = happiness, wellness, neurotransmitter) for sustained remission when applied systematically
- Non-Invasive Vagus Nerve Stimulation
Stimulate Vagus Nerve in Breath
Breathing Exercise
Take Home Message
- Not a “new’ diagnosis, but has changed over time
- Tell your brain “good job” and “you are safe”
- Increased visual dependency = less somatosensory reweighting
- Has central (brain) rewiring component
- Intervention: Vestibular Rehabilitation Therapy (VRT), Cognitive Behavioral Therapy (CBT) and medication
Resources
Brandt T. Vertigo. Its multisensory syndromes. Springer Verlag, New York, 1991.
Brandt T, Dieterich M, and Strupp M. Chapter 5: Psychogenic forms of vertigo and dizziness in “Vertigo And Dizziness: Common complaints: Springer, 1995
Breslau, N., L. R. Schultz, et al. (2000). “Headache and major depression: is the association specific to migraine?” Neurology 54(2): 308-313.
Clark DB, Hirsch BE, Smith MG, Furman JMR, Jacob RG. Panic in otolaryngology patients presenting with dizziness or hearing loss. Am J Psychiatry 1994; 151:1223 1225.
Clark, M. R. and K. L. Swartz (2001). “A conceptual structure and methodology for the systematic approach to the evaluation and treatment of patients with chronic dizziness.” J Anxiety Disord 15(1-2): 95-106.
More Information about PPPD
PPPD Explained article by The Dizzy Cook
PPPD Information from Vestibular Disorders Association (VeDA)

Morgan Kriz, DPT
Vestibular Physical Therapist
Morgan has a Doctorate of Physical Therapy that specializes in Balance and Vestibular Rehabilitation. Morgan does have a strong background in Orthopedic Physical Therapy and this provides a foundation for general musculoskeletal conditions that may contribute to balance limitations.
Her focus as a provider is for patients to feel empowered with management of their condition and learn strategies to live a functional life so they can participate in the things they love. The human body is a magnificent. Each body system has a distinguished function however all systems are interdependent with one another. Morgan tries her best to educate patients so they may be proactive in their healthcare and strives to communicate well with other providers to give efficient and quality care through a multidisciplinary approach.
Vestibular Rehabilitation is an exercise based therapy program used to treat balance and dizziness disorders. It is based on the body’s natural ability to compensate for balance problems through optimizing the brain’s connection from your inner ear; eyes and body. Morgan uses evidence based guidelines when creating a patient’s individualized plan of care for Vestibular Rehabilitation. Morgan believes getting the most out of life is to make it fun/play games and tries to incorporate this into her rehabilitation programs so the brain retains the information for long-term management.
Contact Morgan:
www.pugetsoundent.com/vestibular-rehabilitation
Vestibular Therapy Specialists, telehealth services: www.vestibularspecialists.com
*******
Presentation information is not meant to be taken as medical advice.
Presentations posted online may include discussion notes, links, images, and other information added by Seattle Dizzy Group.
*******
© Copyright 2019, Seattle Dizzy Group. All rights reserved.







Thanks you for sending- this was such an informative presentation. Cheryl
>>
By: Cheryl Petterson on December 2, 2019
at 12:05 pm
[…] In 2019, we had guest speakers on the topics of “Cervicogenic Dizziness” and “Functional Neurology & Neuroplasticity” as well as “Persistent Postural-Perceptual Dizziness (PPPD)“ […]
By: Take A Step Towards Balance In 2020 | Seattle Dizzy Group on January 31, 2020
at 7:43 pm
For years, Meniere’s disease controlled my life with constant dizziness, ringing, and vertigo. Nothing helped until a friend recommended Earthcure Herbal’s treatment. Skeptical but hopeful, I gave it a try. Within weeks, my symptoms eased dramatically. The vertigo faded, the ringing quieted, and I finally felt steady again. Months later, even my doctors were amazed. Earthcureherbalcure. com didn’t just relieve my symptoms, they gave me back my balance and my life. …
By: Harper Thomas on July 5, 2025
at 5:45 am