
Treating & Managing Vestibular Disorders
by Meredith Mancuso, DPT
of MOSAIC Physical Therapy
(Presented to Seattle Dizzy Group on 7/12/14)
This presentation gives an overview of Vestibular Rehabilitation Therapy (VRT) focusing on the treatment of Vestibular Unilateral Hypofunction (as from Meniere’s Disease, Labyrinthitis, or Vestibular Neuritis), and the importance of Gait Speed. 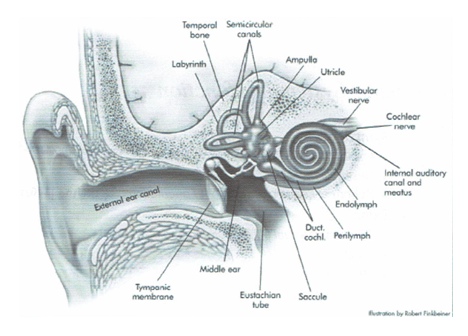
BRIEF ANATOMY AND SYSTEM REVIEW
What does our Vestibular System do?
- Interprets orientation in space
- Interprets linear acceleration
- Interprets rotational acceleration
- Helps us achieve true vertical
What are the important components?
- Otoliths are for the linear acceleration
- Horizontal versus vertical
- Canals are for rotational and filled with fluid called endolymph
- Canals are responsible for BPPV (aka the “dreaded crystals”)
WHAT IS VESTIBULAR HYPOFUNCTION?
- A diagnosis of unilateral vestibular hypofunction is made when the balance system in your inner ear (peripheral vestibular system) is not working properly.
- The system can also be affected on both sides (bilateral hypofunction).
- This typically results from a cold or flu (viral). It could also be due to trauma or surgical intervention. The infection can be bacterial, but this occurs less often.
- This infection can affect, and cause, inflammation of the labyrinth or the nerve.
- Nerve = vestibular neuritis
- Labyrinth = Labyrinthitis
What are the complaints?
- The onset is usually sudden and potentially severe and corresponds with a recent illness.
- Dizzy! With turning head one side or the other.
- Off Balance: Difficulty walking in complex environments such as uneven surfaces or in complex visual fields such as in the grocery store.
- Difficulty with low light situations.
- Often will have complaints of nausea.
- If the labyrinth is involved there may be Hearing changes and sensitivity to loud noises.
How do we know if we have hypofunction?
- Physical therapist or Medical specialist can perform several tests.
- PTs usually use a head thrust test or a dynamic visual acuity test.
- An eye exam is usually performed as well to see if it is acute or if the patient has already learned to compensate.
- Assess Balance.
What do we do about it now?!
- Visit a specialist to rule out more.
- Gaze stabilization exercises – create an error signal to allow change in the brain (compensation).
- X1 viewing – target is in front of you, moving your head at 2hz pace back and forth.
- X2 viewing.
- Incorporate balance and walking with the above tasks.
- Balance exercises that challenge us 3x beyond what we need to be physically capable of doing.
- One method of predicting outcomes and determining if a balance program is effective is to measure and monitor gait speed.

GAIT SPEED
Why do I care?
- Forecast rehabilitation outcomes
- Correlated with:
- Fear of falling
- Gait behavior, such as how successfully an elderly individual can enter the community and cross the street
- Can also predict functional decline
Additional factors that affect Gait Speed
- Motor control and muscle performance affect
- Sensation
- Perception
- Endurance levels
- Environmental characteristics
- Motivation
- Mental health, and cognitive status
What numbers are important?
- Patients who ambulate at speeds slower than 1 m/s benefit from fall prevention training
- Those who walk slower than 0.6 m/s have a high risk of physical disability
- Gait speeds less than 0.6 m/s are also predictive of a future risk of hospitalization and a decline in health and function
- Those who walk faster than 0.8 m/s are characterized as community ambulators and can maneuver through crowds and shopping centers
- The minimum detectable change value of gait speed in patients who lack normal gait speed is 0.1 m/s. In geriatric patients I have seen .05m/s

 Ideas for improvement in Gait Speed
Ideas for improvement in Gait Speed
- Stay flexible! – you have to be able to move to move quickly.
- Range of motion at the hip, particularly into extension (leg behind you) will affect your ability to create a long stride.
- Ankle range of motion and strength are required for push off and to compensate for any loss of balance.
- Stay strong! – build and maintain muscle mass.
- To build muscle you need to be working at an exertion level of about 15 on a scale that goes from 6-20 (rate of perceived exertion).
- Count your steps and see if you can do it in fewer steps.
- This will help improve step length.
- Try to practice dual task activities to boost our ability to multi task when in a controlled environment.
- Counting backwards
- Carrying water
- Singing
- Incorporate visual distractions.
- Try pushing and pulling an item, particularly if you are working towards walking with a pet.
- Try changing the surface.
- Change the light source or close your eyes (perform safely please!).
See also: “Vestibular Physical Therapy for Dizzy Patients”
 Meredith Mancuso, DPT
Meredith Mancuso, DPT
of MOSAIC Physical Therapy
Meredith grew up in Boston, MA. She attended Colby College in Waterville, ME and went on to get her Doctorate in Physical Therapy at Massachusetts General Hospital’s Institute of Health Profession, Boston, MA. She joined MOSAIC PT in March 2014.
http://www.mosaicrehab.com/mlt/therapists/meredith_mancuso.php
VRT Image from: www.mosaicrehab.com
*******
Presentation information is not meant to be taken as medical advice.
Presentations posted online may include discussion notes, links, images, and other information added by Seattle Dizzy Group.
(Join the Seattle Dizzy Group closed/secret Facebook group to download the presentation. Send us your email address for invitation to join our Facebook group).
*******







[…] Treating and Managing Vestibular Disorders (seattledizzygroup.org) […]
By: Simple exercises are an easy and cost-effective treatment for persistent dizziness – “vestibular rehabilitation” or “balance retraining” « Clinicalnews.org on August 25, 2014
at 1:06 am
[…] Treating and Managing Vestibular Disorders […]
By: Treating Dizziness and Imbalance with Physical Therapy | Seattle Dizzy Group on October 31, 2017
at 11:57 pm